Toni Susin
Last modified 03/04/2013
Menu:
SIMULATION OF THE HUMAN INGUINAL REGION:
Researches: Gerard Fortuny, Manuel López-Cano, Antonio Susin.

Description:
The possible cause of inguinal hernias in adults is multiple. The combination of altered collagen metabolism and changes of the anatomic structural characteristics of the inguinal region may distort the physiological mechanisms of contention of the abdominal viscera [Ab01]. The repair of an inguinal hernia is one of the most common operations performed by general surgeons in Western countries [Ru98]. The success of groin hernioraphy seems to be influenced by the specific technique of repair used and by surgeon-dependent factors, such as specific training, interest, and skills [McG98]. Technical ability is indeed a very important dimension in surgical education. However, it has been shown that teaching basic surgical skills in the operating room is not efficient and carries high costs [Pe01].
Rapid advances in engineering, computer science, and imaging technologies had also revolutionized the field of surgery. New procedures utilizing robotic, computer-assisted, and image-guided systems are moving from the laboratory to clinical practice. Virtual reality (VR) surgical simulation increasingly appears to be a promising aspect of the surgical education process. Three-dimensional visualization of the human inguinal region could be of great help to appreciate dynamically and objectively the physiological mechanisms protecting against the development of a hernia and the influence of anatomic variations on the functioning of the inguinal defence mechanisms, to allow planning and realistic surgical simulation of groin hernia repair, to practice a given gesture or procedure repeatedly, etc. On the other hand, review of performance after completion of the skill is critical in improving overall surgical capabilities.
 The final goal of this task is two fold: first to build a VR simulator for helping in surgeons training, and second, to be able to simulate the inguinal human region in motion (almost every present known data is static) in order to understand the possible causes for an inguinal hernia to appear.
The final goal of this task is two fold: first to build a VR simulator for helping in surgeons training, and second, to be able to simulate the inguinal human region in motion (almost every present known data is static) in order to understand the possible causes for an inguinal hernia to appear.
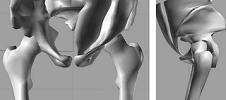
Fig 2. Semiautomatic segmentation of the different anatomical structures.
The first step would be to build a 3D model of the inguinal region using data from the Visible Human Project [VHP] in order to obtain an anatomical correct model. The most important anatomic unities in this region are the pelvic bone, the rectus abdominis muscle, the external and internal oblique muscles, the transverse muscle of the abdomen, the aponeurosis of these muscles, and the spermatic cord. The segmentation will be done in a semi-automatic process due to that insertion parts of the muscles and aponeurosis are not well identified using contrast in the VHP images, anatomical references will be used for completion of the model. The final 3D model has to be parametrical in order to incorporate some of the real anatomical measurements that surgeons have collected.

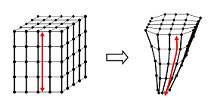
Fig 3. Muscle deformation under external forces running on the GPU.
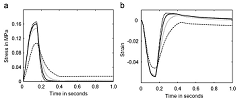
As a first approach muscles can be animated by a deformable model that allows realistic real-time response to user interaction, possibly using mass-spring. For research purposes, but renouncing to real-time, we will also build a more complex dynamical model based on a visco-elastic approach that includes biochemical parameters responsible of changes in the elastic properties of the muscle fibres [LMH05]. These changes are suspect to play an important role when an inguinal hernia appears.
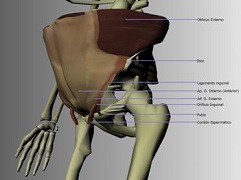
Fig. 4. Anatomical muscle model of the inguinal region.
For this complete task we have the support of the abdominal surgeon team of the Hospital de la Vall d’Hebron (Barcelona).
Fortuny G, Susin A, Lopez-Cano M. Simulation and study of the geometric parameters in the inguinal area and the genesis of inguinal hernias. Computer Methods in Biomechanics and Biomedical Engineering, March 2011. (Online DOI:10.1080/10255842.2010.522182)

Fortuny G, Rodriguez-Navarro J, Susin A, Lopez-Cano M. Simulation and study of the behaviour of the transversalis fascia in protecting against the genesis of inguinal hernias. Journal of Biomechanics, Vol 42, pp 2263-2267, 2009
Fortuny G, Rodriguez-Navarro J, Susin A,.Armengol-Carrasco M., Lopez-Cano M. A simulation finite element model for the mechanics of the internal oblique muscle: A defense mechanism against inguinal hernia formation? Computers in Biology and Medicine, Vol 39, pp 794-799, 2009

Lopez-Cano M, Fortuny G, Rodriguez-Navarro J, Susín A., Armengol-Carrasco M. Raymond C. Read (2007) Arthur Keith, the anatomist who envisioned herniosis. Hernia, Vol 12 (3) pp 331-331, 2008
G. Fortuny, A. Susín, M. López-Cano, J. Marcé Simulation with FEM to describe the dynamic of the inguinal area: the shutter mechanism. Journal of Biomechanics, Vol 41, pp S375-S376, 2008
López-Cano M., Rodríguez-Navarro J., Rodríguez-Baeza A., Armengol-Carrasco M., Susín A. A real-time dynamic 3D model of the human inguinal region for surgical Education.Computers in Biology and Medicine, vol 37 (9), pp 1321-1326, 2007.
López-Cano M., Rodríguez-Navarro J., Rodríguez-Baeza A., Armengol-Carrasco M., Susín A.
A real-time dynamic 3D model of the human inguinal region for surgical Education.
Computers in Biology and Medicine, In Print., 2007
López-Cano M., Rodríguez-Navarro J., Susín A.
Modelización Dinámica de Hernia Inguinales.
Jornada Matemáticas / "Industria" de la FECYT. Sesión sobre "Matemáticas en las Ciencias de la Salud". Univ. Complutense de Madrid . 2005.
References:
[Ab01] Abrahamson J., Mechanisms of hernia formation. Bendavid R, Abrahamson J, Arregui ME, Flament JB, Phillips EH (eds). Abdominal wall hernias: Principles and management. New York: Springer-Verlag, 2001:133−137.
[Be00] Bestel J.. Modèle différentiel de la contraction musculaire contrôlée. Application au système cardiovasculaire.PhD thesis, Universitée Paris-Ix Dauphine, 2000.
[Fu93] Y.C. Fung. Biomechanics: Mechanical properties of living tissues. Springer-Verlag, New York, 1993.
[MCT98] Marescaux J, Clément JM, Tassetti V, Koehl C, Cotin S, Russier Y, Mutter D, Delingette H, Ayache N. Virtual reality applied to hepatic surgery simulation: the next revolution. Ann Surg 1998; 228:627–634.
[McG98] McGreevy JM. Groin hernia and surgical truth. Am J Surg 1998; 176:301−304.
[Pe01] Peracchia A. Surgical education in the third millennium. Ann Surg 2001; 234:709−712.
[LMH05] López-Cano M, Munhequete EG, Hermosilla-Pérez E, Armengol-Carrasco M, Rodríguez-Baeza A. Anthropometric characteristics of the pubis arch and proper function of the defense mechanisms against hernia formation. Hernia 2005; 9:56−61.
[Ru98] Rutkow IM. Epidemiologic, economic, and sociologic aspects of hernia surgery in the United States in the 1990s. Surg Clin North Am 1998; 78:941−951.
[SW98] Spitzer VM, Whitlock DG. The visible human data set: the anatomical platform for human simulation. Anat Rec (New Anat) 1998; 253:49–57.
[VHP] http://www.nlm.nih.gov/research/visible/visible_human.html
[ZM90] G.I. Zahalak and S.P. Ma. Muscle activation and contraction - constitutive relations based directly on cross-bridge kinetics. Journal of Biomechanical Engineering, 112(1):52--62, 1990.